In recent years, periodontal treatment has increasingly followed the clinical framework “Treatment of Stage IV Periodontitis: The EFP S3 Level Clinical Practice Guideline” outlined by the European Federation of Periodontology (EFP).
In response, NSK is proud to introduce M.I.T. our new initiative aligned with the global standard. Through M.I.T., NSK provides both products that support periodontal treatment and opportunities for learning and discovery related to periodontal care.
Join us
M.I.T. aligns with the benchmark in periodontal treatment – being anchored in the EFP S3 Level Clinical Guidelines and built around a patient-first philosophy. This modern approach empowers clinicians to deliver precise, predictable, and evidence-based care for stage I–III periodontitis.
By embracing this structured, research-driven framework, clinicians can elevate their practice, enhance patient outcomes, and align with global standards in periodontal care. This framework empowers clinicians to deliver effective, evidence-based care through three key pillars:

Accurate diagnosis is the foundation of successful treatment. Clinician begin by checking their patient's risk factors (systemic, local and lifestyle factors). Conduct a full intraoral and extraoral exam/analysis. Initiate patient engagement.

Clinicians establish a diagnosis and conclude with a personalised treatment plan, based on the patient's unique case. Personalised care can be provided using NSK’s extensive portfolio of precision instruments and technologies – designed to support clinicians and patients in every stage of periodontal therapy.

Patients are equipped with the knowledge and education to maintain their oral health independently. Through patient engagement, with the support of clinicians and NSK solutions, long-term outcomes become a shared achievement.


All patients should first undergo a comprehensive consultation and clinical examination, so that dental professionals can establish an accurate diagnosis, determine the appropriate evidence-based treatment plan, and provide patient-centred education according to the individual’s unique condition.

Periodontal care is a cornerstone of oral health – essential for every patient, regardless of symptoms. Step 0: Screen / Assess applies universally, from first-time visitors to patients in long-term maintenance, ensuring that every individual receives a personalised and evidence-based treatment approach, according to their condition at the time of each treatment.

Before any treatment begins, a comprehensive evaluation is essential. This includes a multidimensional assessment of the patient’s oral health, systemic conditions, lifestyle habits, and risk factors. Based on this thorough analysis, we establish a diagnosis grounded in scientific evidence and clinical best practices. The goal is clear: to formulate a treatment plan that is precisely tailored to the individual needs of each patient. Step 0 is more than a starting point – it is the core of clinical excellence. By embracing this approach as a unified team and integrating it into daily practice, we elevate the quality of care, enhance patient satisfaction, and achieve long-term treatment success.

Assess the patient’s current condition, using periodontal charts (pocket/probing depths, bleeding on probing (BoP), clinical attachment level (CAL) measurements, and biofilm scores), as well as appropriate radiographs.

Explain the intention of a minimally invasive approach (and possibly introduce the M.I.T. framework). Identify what treatment pathway the patient is currently on and discuss it with them to ensure understanding and engagement.

Step 1 focuses on behaviour change and supragingival biofilm control, personalised oral-hygiene education (e.g. toothbrushing and interdental cleaning), PMPR (Professional Mechanical Plaque Removal), correction of plaque-retentive factors, and targeted risk-factor control (e.g. smoking cessation and glycaemic control). The aim is to engage and motivate the patient, ultimately creating a patient-maintainable environment before any subgingival therapy.
Step 1 covers most types of patients, specifically patients with gingival health, gingivits, periodontitis, peri-implant health, peri-mucositis, and/or peri-implantitis. Patients might for example present gingival inflammation, characterised by erythema, edema, and bleeding on probing. Plaque control might be inadequate, and the patient might yet need to establish consistent oral hygiene habits. Supragingival plaque and calculus could be heavily accumulated, and systemic risk factors such as smoking or diabetes may be contributing to the periodontal condition.
The key goal is to disrupt biofilm, remove plaque retentive factors such as staining, reduce inflammation and achieve patient engagement – as deemed relevant. Supragingival plaque and calculus can be effectively eliminated to prevent an early inflammatory response and establish a healthy periodontal environment.

Patients may be treated by supragingival/mucosal biofilm disruption, PMPR (Professional Mechanical Plaque Removal) and plaque retentive factor management. Common treatment mechanisms are for example, powder therapy, piezo ultrasonic scaling / air scaling, hand-instrumentation, polishing, and the use of rotary instruments (to manage plaque retentive factors).

If healthy: Repeat Step 0/1
If stable: Step 4
If unstable & engaged: Step 2
If unstable & non-engaged: Repeat Step 1

Varios Combi Pro2

Powders Perio Mate Powder, FLASH pearl & SOFT pearl

Prophy-Mate neo Powder Handpiece

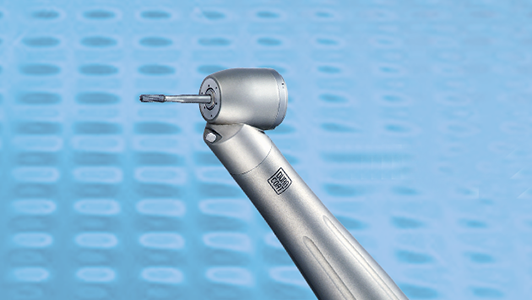
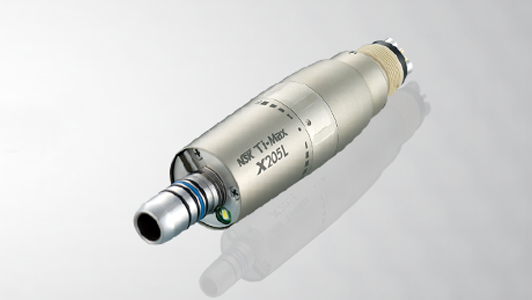
VA2-LUX-HP Ti Piezo Scaler Handpiece

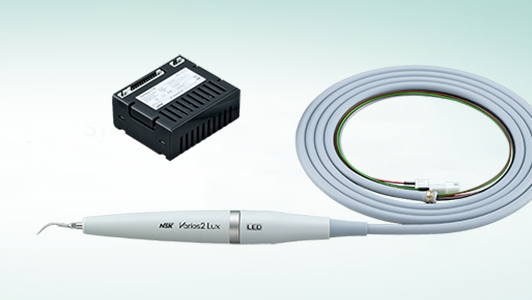
Varios 970 Piezo Scaler
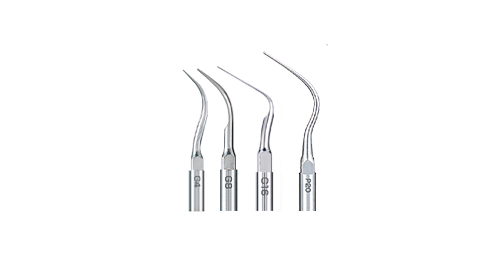
Piezo Scaler Tips G4, G8, G16 & P20

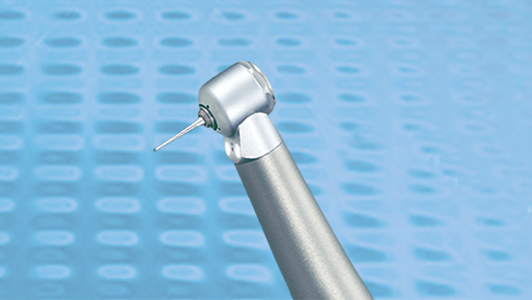
Ti-Max S970 Air Scaler
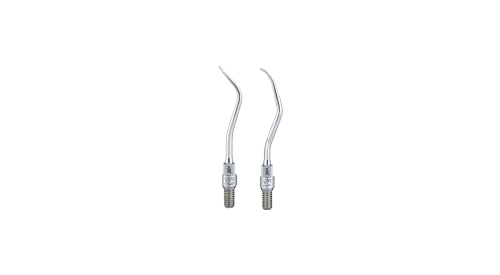
Air Scaler Tips S3 & S1

iProphy

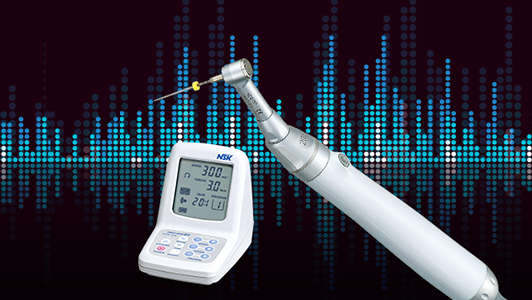
Ti-Max Z25L Rotary instrument
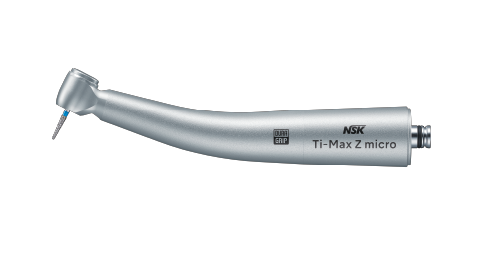
Ti-Max Zmicro Rotary instrument

Step 2 focuses on subgingival instrumentation, removing subgingival biofilm and calculus and aiming to reduce bleeding and pocket depth(s) without surgery. High-quality instrumentation and reassessment is key during this phase.
The patient might present with:
Periodontitis: Periodontal inflammation with progressive loss of periodontal ligament and alveolar bone, resulting in clinical attachment loss (CAL) and periodontal pocketing (often with bleeding on probing and/or suppuration). Left untreated, it could lead to tooth mobility and potential tooth loss.
Peri-mucositis: A reversible, plaque-associated inflammatory lesion confined to the peri-implant soft tissues, presenting with bleeding on probing (suppuration), erythema and oedema, without radiographic bone loss beyond initial post-placement remodelling.
Peri-implantitis: Inflammation of the mucosa together with progressive loss of supporting crestal bone compared with a baseline, typically accompanied by increased probing depths and bleeding on probing and/or suppuration. Without intervention, implant failure is likely.
Effective removal of subgingival biofilm and calculus to reduce periodontal pocket inflammation, promote soft tissue healing, and achieve pocket depth reduction – establishing a foundation that lowers the likelihood of future surgical intervention. The removal of plaque retentive factors such as overhangs might be necessary and continued patient engagement remains essential.
Patients may be treated by subgingival/submucosal biofilm disruption. Common treatment mechanisms are for example powder therapy, piezo ultrasonic scaling / air scaling, and/or hand-instrumentation.
If stable: Step 4
If unstable: Repeat Step 2, or move to Step 3

Step 3 targets residual deep sites and hard-to-clean defects, using site-specific corrective therapy to gain access for thorough decontamination and to reshape or regenerate tissues where indicated. This may include resective or regenerative periodontal surgery and periodontal plastic procedures, selected to stabilise the periodontium and improve long-term maintainability.
The patient continues to show sites which does not sufficiently improve with continued treatment from non-surgical therapy (Step 1 & Step 2). These areas of incomplete healing indicate a need for surgical intervention / targeted procedures after Step 2, to correct persistent pocketing and restore proper periodontal architecture.
The goal is to eliminate or reduce periodontal pockets and restore osseous defects – ultimately stabilising active disease, supporting long-term tooth preservation and functional rehabilitation.

Treatment may include: Bone remodelling, bone regeneration, and/or hard and soft tissue grafts.
If stable: Step 4

Step 4 focuses on supportive periodontal care (maintenance)—a lifelong, risk-based programme of periodic review, monitoring (e.g., bleeding on probing, pocket depths, stability), and tailored prevention to sustain health and prevent recurrence. It reinforces home care and risk-factor control (e.g., smoking, glycaemic management) and provides professional prophylaxis and targeted retreatment of sites as indicated to maintain stability over time.
The patient’s periodontal tissues are clinically stable, showing little to no inflammation. Pocket depths are shallow, with no bleeding on probing or signs of infection. The patient follows excellent oral hygiene routines and remains highly motivated. Ongoing supportive periodontal therapy helps effectively prevent disease from returning.
Maintain periodontal stability post-treatment and prevent disease recurrence through ongoing supportive care. Patients are empowered to sustain effective oral hygiene and lasting motivation, while facilitating early detection and timely intervention – all key to ensuring long-term tooth retention.

Patients may be treated by supragingival/mucosal biofilm disruption, PMPR (Professional Mechanical Plaque Removal) and plaque retentive factor management. Common treatment mechanisms are for example, powder therapy, piezo ultrasonic scaling / air scaling, hand-instrumentation and polishing.
Schedule continuing care every 3-12 months (according to the patient’s needs).
A perio patient never ceases to be a perio patient.
M.I.T. supports you and your team as the clinical decision makers as dental professionals and can facilitate a unified understanding within your clinical team for periodontital treatment because:

It is not about applying the same treatment to all patients, but rather placing importance on understanding each patient's unique situation and tailoring the appropriate approach accordingly.

It accommodates a wide range of patients with various conditions and stages of periodontal treatment.
It is patient focused, offering clincial choice and supporting evidence based periodontal care.
"NSK has developed the M.I.T. concept to align closely with the international standards for periodontal therapy outlined in the EFP S3-level clinical practice guidelines. By mapping their devices to all four phases of periodontal care—from non-surgical and surgical interventions to maintenance therapy—while providing clinicians with flexibility of choice, NSK takes an important step toward facilitating the implementation of these standards in everyday clinical practice."